

I’ve treated CEOs who closed seven-figure deals in the morning and detoxed alone at night.
I’ve treated nurses who charted flawlessly while quietly misusing prescriptions to get through 12-hour shifts.
I’ve treated therapists who could articulate attachment theory beautifully — while drinking themselves to sleep.
They were high-functioning.
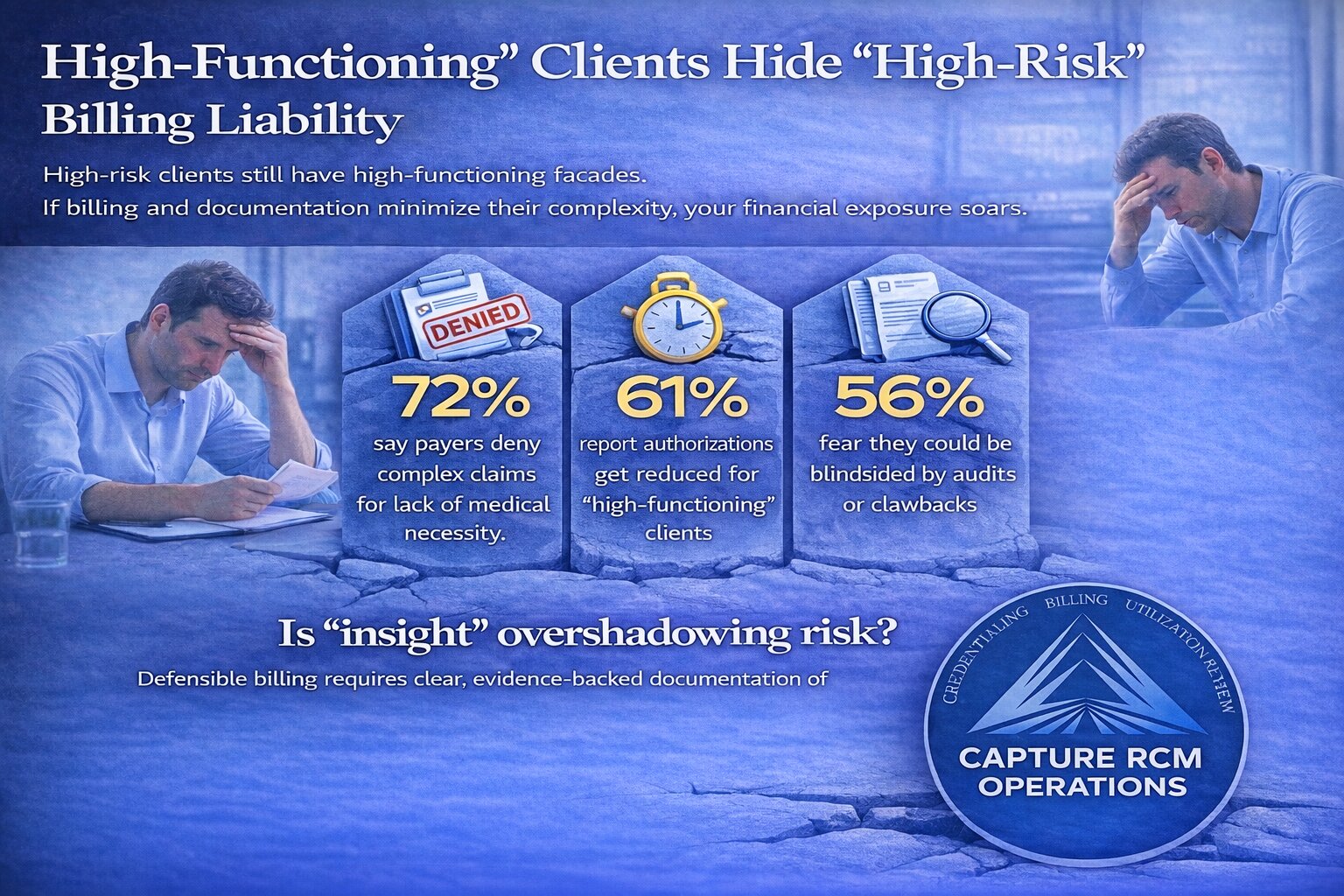
They were also high-risk.
And here’s the part we don’t say out loud enough in operations meetings: if your documentation and billing don’t reflect that risk clearly and consistently, your practice becomes the one carrying the liability.
If you’re running programs built for complexity — especially when mental health and substance use collide — your billing operations can’t be generic.
They have to be as sophisticated as your clinical team.
High-Functioning Is a Presentation — Not a Risk Assessment
High-functioning clients don’t miss appointments.
They don’t slur their words.
They don’t always look “impaired.”
They look tired. Driven. Controlled.
Underneath that control is often:
- Escalating tolerance
- Sleep disruption
- Anxiety masked as productivity
- Depression masked as achievement
- Medical instability masked as resilience
The absence of visible chaos does not equal the absence of clinical severity.
But too often, charts reflect appearance instead of pathology.
When documentation leans on phrases like “client stable,” “client insightful,” or “client motivated” — without clearly linking symptoms to functional impairment — you weaken your own medical necessity argument.
Payers don’t reimburse based on vibe.
They reimburse based on evidence.
The Hidden Cost of Under-Documenting Complexity
High-functioning clients require careful clinical framing.
They may need structured daytime care or multi-day weekly treatment precisely because they haven’t crashed yet. The intervention is preventative — stabilizing before collapse.
But prevention is harder to justify on paper.
If your team documents:
- Insight but not severity
- Compliance but not risk
- Attendance but not impairment
You create a chart that looks outpatient-level — even if you’re providing higher-intensity care.
That mismatch creates three predictable outcomes:
- Authorizations get reduced.
- Claims get denied.
- Audits become dangerous.
And when that happens, providers start second-guessing clinical decisions based on reimbursement pressure instead of patient need.
That’s where integrity erodes.
Not because you don’t care — but because your infrastructure doesn’t protect you.
Burnout + High-Functioning Clients = Documentation Drift
Let’s talk honestly.
Your clinicians are stretched thin.
Your utilization review team is negotiating constantly.
Your biller is chasing down incomplete notes two weeks after session.
High-functioning clients can feel “easier.” They show up. They participate. They articulate goals.
So notes get shorter.
Risk language gets softer.
Functional impairment becomes implied instead of explicitly documented.
That’s documentation drift — and it’s one of the biggest silent revenue leaks in behavioral health.
It’s not fraud.
It’s not negligence.
It’s fatigue.
But fatigue doesn’t protect you in an audit.
Structure does.
Risk Signals You Might Be Underestimating
You might be under-capturing medical necessity if:
- You rely on diagnosis codes without describing day-to-day impairment
- You document “work functioning intact” without exploring emotional or cognitive decline
- You downplay substance quantity because there’s no DUI or hospitalization
- You assume professional status equals stability
- You don’t clearly connect relapse risk to treatment intensity
High-functioning clients are experts at maintaining external structure.
Your documentation must focus on internal destabilization.
That distinction matters.
Payers Scrutinize High Performers More — Not Less
Here’s what many providers don’t realize:
When a client is employed, licensed, or high-income, payers often scrutinize claims more aggressively.
Why?
Because the surface narrative contradicts high-intensity care.
If someone is still managing their law firm, why do they need multi-day weekly treatment?
If someone hasn’t lost their job, why structured daytime care?
You know the answer clinically:
Because collapse is coming.
Because functioning is deteriorating.
Because the strain is unsustainable.
But unless your documentation spells that out — clearly, repeatedly, and consistently — your authorization team is fighting uphill.
Your billing department shouldn’t be reverse-engineering medical necessity after the fact.
It should be aligned from the first intake note.
The Financial Risk of “We’ll Fix It Later”
I see this often with growing programs.
The clinical team is strong. Outcomes are good. Census is rising.
Billing feels “good enough.”
Until:
- A payer requests 12 months of records.
- A recoupment notice arrives.
- An audit questions level-of-care decisions.
- A credentialing gap delays reimbursement.
High-functioning clients, because they often stay longer in care, can create larger recoupment exposure if documentation doesn’t fully justify intensity.
And if your current mental health billing services operate transactionally — posting payments, submitting claims, reacting to denials — you’re missing the strategic layer.
Revenue cycle in behavioral health is compliance management.
Especially when clinical presentations are nuanced.
Clinical Integrity Requires Operational Backbone
When I speak to practice owners, the fear isn’t usually “Will we fill beds?”
It’s:
“Are we exposed?”
“Are we documenting correctly?”
“Are we leaving money on the table?”
“Will this hold up in an audit?”
Those are not small questions.
If you treat high-functioning addiction, your operational model must:
- Ensure accurate CPT alignment with service intensity
- Support clinicians with documentation guardrails
- Strengthen utilization review narratives
- Monitor payer patterns for high-performing demographics
- Protect against clawbacks with internal QA review
That isn’t overkill.
It’s protection.
Because high-functioning addiction hides clinical risk.
Weak revenue systems hide financial risk.
Both show up eventually.
And when they do, they’re rarely gentle.
FAQ: What Providers Ask About High-Functioning Clients & Billing
Why are high-functioning clients harder to justify at higher levels of care?
Because payers often equate visible dysfunction with severity. When clients are employed or socially intact, documentation must clearly describe psychological distress, relapse risk, cognitive impairment, or medical concerns — not just surface stability.
Can we bill higher intensity care if the client hasn’t “bottomed out”?
Yes — if medical necessity is clearly documented. Treatment intensity is based on risk, symptom severity, and functional impairment, not dramatic external consequences. The key is how thoroughly those factors are reflected in the chart.
What’s the biggest documentation mistake with high-functioning addiction?
Overemphasizing insight and compliance while under-documenting instability. Insight doesn’t negate risk. Attendance doesn’t eliminate impairment.
How can billing teams better support clinicians treating complex clients?
By creating documentation templates that prompt risk language, aligning CPT coding with actual service delivery, and reviewing notes proactively — not just when denials occur.
Are audits more common with high-income or licensed professionals?
In many cases, yes. When claims show extended high-intensity care for individuals who appear externally stable, payers may scrutinize more closely. Strong documentation reduces vulnerability.
When should a practice consider upgrading its billing infrastructure?
If you’re experiencing repeated authorization reductions, unexplained denials, delayed reimbursements, or anxiety about compliance — it’s time to assess whether your billing partner is strategic or simply reactive.
You Shouldn’t Have to Choose Between Care and Compliance
You went into behavioral health to treat complexity.
To sit with nuance.
To intervene before collapse.
To hold space for people who look fine and feel anything but.
Your billing infrastructure should protect that work — not undermine it.
If you’re tired of wondering whether your claims accurately reflect the care you provide…
If you’re uneasy about whether your documentation would survive scrutiny…
If you know your high-functioning clients are clinically high-risk and your systems aren’t built for that level of precision…
It’s time to tighten the backend.
Call 380-383-6822 or visit our mental health billing services to learn more about our behavioral health billing services.