

I used to think our outcomes were the issue.
Cancellations. Early discharges. Clients saying, “This just didn’t work for me.”
It felt like a treatment problem.
It wasn’t.
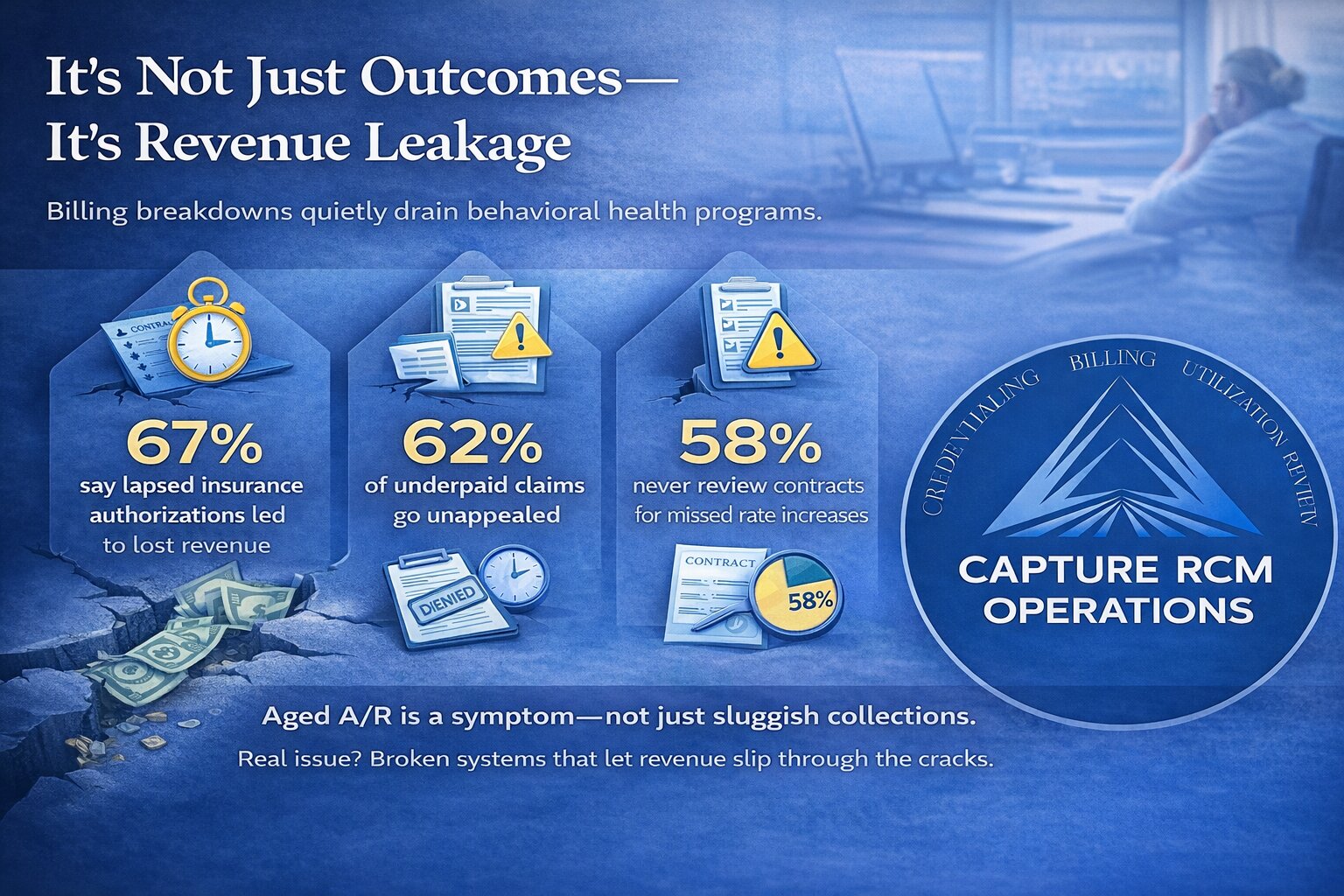
It was revenue leaking out the back door—and I didn’t even know it.
Within the first few months of reviewing our numbers and looking seriously at our behavioral health billing support, I realized something uncomfortable:
We weren’t struggling because care didn’t work.
We were struggling because we weren’t getting paid correctly—or consistently—for the care we were already providing.
And once I saw it, I couldn’t unsee it.
I Thought Clients Were Quitting. Some Were Just Losing Coverage.
When a client stopped coming, I assumed disengagement.
When insurance stopped approving sessions, I assumed that was just how it goes.
But when we finally did a deeper audit, the story shifted.
Authorizations weren’t always extended before they expired.
Re-verifications weren’t happening on time.
Documentation didn’t always match payer nuances.
It wasn’t laziness. It wasn’t incompetence. It was overload.
Our front desk was juggling phones, intake, scheduling, and benefits checks. Our clinicians were charting at night. Our biller was doing her best—but she was one person.
To the client, it felt like instability.
To us, it felt like noise.
But that “noise” was revenue slipping through cracks.
I Blamed Engagement. It Was Actually A/R Aging.
When revenue dipped, I went straight to the clinical team.
“Do we need better programming?”
“Are groups strong enough?”
“Is the curriculum resonating?”
Meanwhile, our accounts receivable was quietly stretching past 60… then 90… then 120 days.
Denials were sitting untouched.
Underpayments weren’t appealed.
Claims were submitted, but not aggressively followed through.
We weren’t failing clinically.
We were under-collecting operationally.
That realization stung. Because it meant the problem wasn’t philosophical. It was structural.
And structural problems require systems—not inspiration.
The Stress Was Bleeding Into Leadership
No one talks about this part enough.
When your cash flow is inconsistent, you start leading from anxiety.
You hesitate to hire.
You delay raises.
You question expansion.
You overreact to normal census fluctuations.
And slowly, you start doubting your entire model.
I remember thinking, “Maybe this level of care just isn’t sustainable.”
It wasn’t the level of care.
It was the back office.
Once I understood how critical strong mental health billing services actually are, I realized we had been treating revenue cycle management like a side task instead of a clinical support function.
And that was costing us more than money. It was costing us clarity.
“Treatment Didn’t Work” Sometimes Means “The System Was Disorganized”
This part hit hardest.
We had former clients say treatment “didn’t work.”
At first, I internalized it as a reflection on programming.
But when we looked closer, patterns emerged:
- Surprise balances because benefits weren’t fully verified
- Confusion about what insurance would cover
- Mid-program authorization lapses
- Delays in claim processing that created billing tension
When the financial experience feels chaotic, it erodes trust in the clinical experience.
Clients don’t separate those things. To them, it’s one ecosystem.
If billing feels unstable, the program feels unstable.
And skepticism grows.
The Revenue I Didn’t Know I Was Losing
Here’s what surprised me most: there wasn’t one catastrophic mistake.
It was death by a thousand paper cuts.
- Claims paid below contracted rates
- Modifiers missing
- Credentialing applications stalled
- Timely filing limits quietly expiring
- Secondary insurance never billed
- No consistent denial tracking dashboard
Individually? They felt manageable.
Collectively? It was tens—eventually hundreds—of thousands in recoverable revenue over time.
Revenue we had already earned.
Revenue tied to care we had already delivered.
Revenue that could have stabilized staffing, improved benefits, funded training, and reduced burnout.
That’s when I stopped seeing billing as “administrative.”
It’s operational oxygen.
The Shift: Treating Revenue Like a Clinical Priority
The turning point wasn’t dramatic.
It was disciplined.
We stopped asking, “Did we submit it?”
And started asking, “Was it paid correctly?”
We stopped accepting denials at face value.
We tracked patterns.
We stopped assuming benefits checks were simple.
We standardized verification workflows.
We looked at credentialing timelines like expansion strategy—not paperwork.
And we partnered with specialists who live and breathe this work.
The result?
- Cleaner claims
- Faster reimbursements
- Fewer write-offs
- Predictable cash flow
- Less staff burnout
But more importantly:
We stopped questioning our worth every time revenue dipped.
Because we finally understood what was clinical fluctuation—and what was operational leakage.
What I’d Tell Any Skeptical Program Owner
If you’ve ever thought:
- “Maybe our outcomes just aren’t strong enough.”
- “Maybe insurance reimbursement is just bad everywhere.”
- “Maybe this is as good as it gets.”
Pause.
Have you audited:
- Your denial rates?
- Your average reimbursement by payer?
- Your authorization lag times?
- Your credentialing timelines?
- Your A/R aging buckets?
- Your underpayment tracking?
If not, you don’t have a treatment problem yet.
You have a visibility problem.
And visibility changes everything.
FAQs About Revenue, Billing, and Stability in Behavioral Health
How do I know if I’m losing revenue without realizing it?
Look at your A/R aging report first. If more than 20–25% of your receivables are over 90 days, there’s likely follow-up breakdown.
Also review:
- Denial rates by payer
- Average reimbursement per CPT code
- Write-off percentages
- Timely filing losses
If you’re not reviewing these monthly, revenue leakage is almost guaranteed.
Isn’t some level of denial normal?
Yes. But unmanaged denial is not.
A healthy operation tracks denial categories, identifies trends, and implements corrective action quickly.
If denials are being “written off” instead of analyzed, that’s lost revenue—not unavoidable friction.
We’re small. Do we really need specialized support?
Small programs feel revenue gaps the hardest.
When you have thin margins, even minor underpayments compound quickly.
Strong mental health billing services aren’t just for large organizations. In many cases, smaller providers benefit even more because they don’t have in-house redundancy.
How does billing impact client retention?
Clients experience billing as part of care.
If:
- Benefits are unclear,
- Bills are inconsistent,
- Coverage changes mid-treatment,
- Or staff can’t answer insurance questions confidently,
Trust erodes.
Clear, consistent financial communication improves retention—because clients feel stable.
What’s the first operational metric I should review?
Start with:
- A/R aging
- Net collection rate
- Denial percentage
- Average days in A/R
Those four numbers alone can reveal more about financial health than census alone.
How long does it take to stabilize revenue once systems improve?
It depends on backlog.
Most programs see measurable improvement in:
- Denial resolution within 30–60 days
- Cash flow stabilization within 60–90 days
- Long-term predictability within 4–6 months
Consistency is key. Revenue cycle improvements compound over time.
Is outsourcing billing giving up control?
Not if done correctly.
The right partner increases transparency. You should have more visibility, clearer reporting, and stronger accountability—not less.
Control isn’t about doing everything yourself.
It’s about having accurate data and predictable systems.
If you’ve been questioning whether your program “works,” don’t rush to rewrite your curriculum.
Look at your infrastructure.
You might be sitting on earned revenue that simply hasn’t been recovered.
And you don’t have to figure it out alone.
Call 380-383-6822 or visit our billing services page to learn more about our mental health billing services.