

Aging A/R isn’t just a line on a spreadsheet—it’s a signal of deeper system inefficiencies. For Billing Directors in behavioral health organizations, improving cash flow isn’t just about better collections—it’s about eliminating preventable losses. The problem? Many of those losses are baked into the process long before a claim is submitted.
If you’re struggling with stagnant revenue, increasing write-offs, or month-over-month A/R growth, the issue likely isn’t volume—it’s leakage. And it’s fixable.
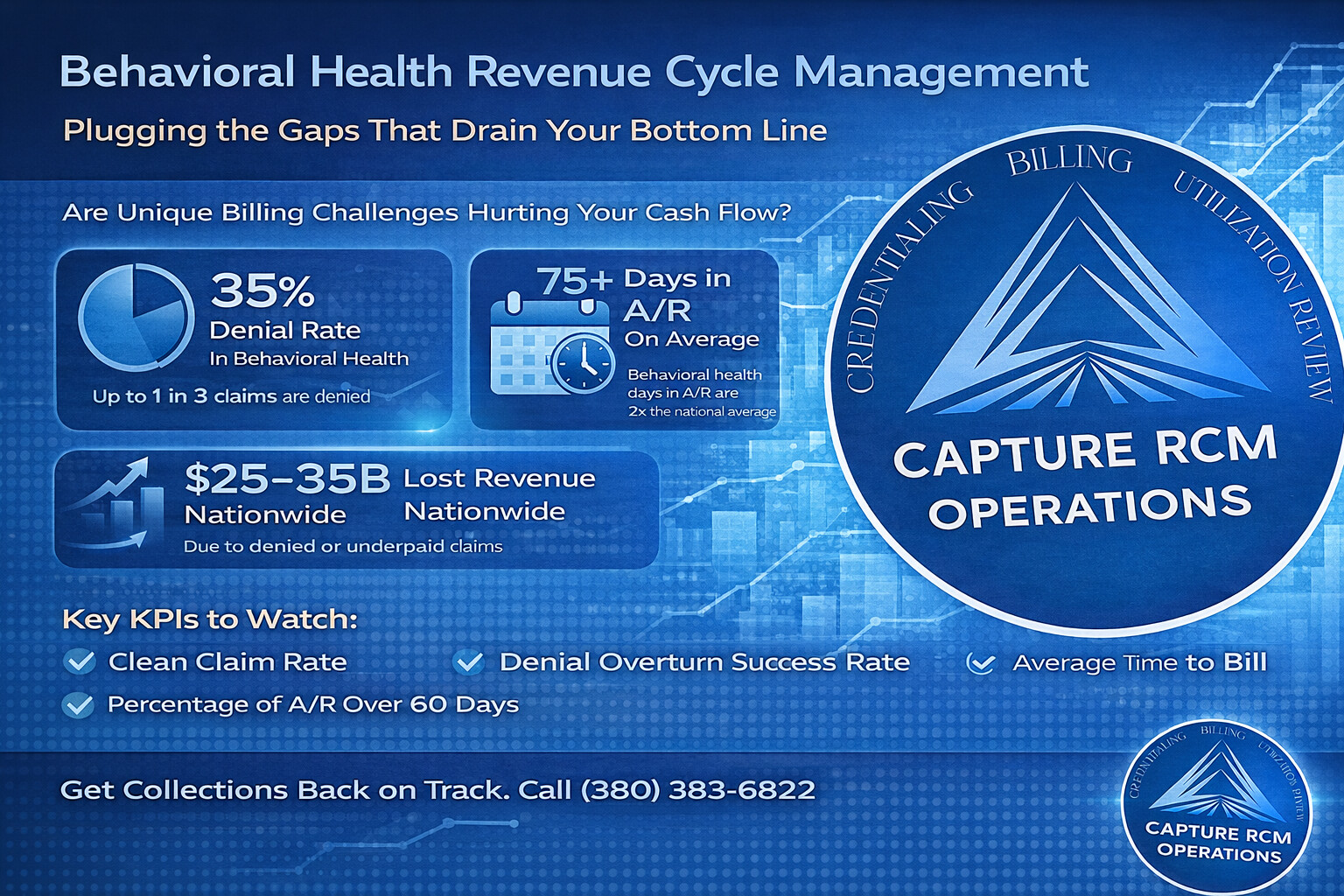
At Capture RCM, we specialize in behavioral health revenue cycle management that closes gaps, recovers revenue, and gives Billing Directors a clear path to efficiency.
1. Front-End Errors Are Slowing Cash Before It Starts
The Problem:
Most claims are doomed from the start because of incorrect or incomplete patient data, missing pre-authorizations, or real-time eligibility failures.
Why It Matters:
According to MGMA, up to 65% of denied claims are never reworked—many of which stem from front-end mistakes. Each one of those denials could have been prevented with better intake execution.
Plug the Gap:
- Build a structured intake checklist for insurance verification, authorization, and coverage windows.
- Use digital tools to flag incomplete data in real time.
- Train front-desk staff monthly on payer-specific policies—especially for Medicaid and out-of-state plans.
2. Documentation Lags Lead to Costly Delays or Denials
The Problem:
Therapist notes submitted days late. CPT modifiers inconsistently used. Missing session dates. Incomplete documentation creates delays in billing and invites audits.
Why It Matters:
Behavioral health payers are tightening documentation standards across the board. When notes are late or noncompliant, claims sit idle or get rejected outright.
Plug the Gap:
- Implement a compliance-aware EMR workflow that forces completion before submission.
- Pair clinical and billing teams on documentation audits.
- Consider pre-submission review tools that catch red flags (like missing time-based elements or mismatched CPT codes).
3. Manual A/R Follow-Up Wastes Time and Misses Patterns
The Problem:
Many billing departments still rely on manual tickler systems or spreadsheets to track claim status and follow-ups.
Why It Matters:
Without workflow automation and intelligent segmentation, follow-up becomes reactive—focused on what’s urgent rather than what’s impactful. This leads to longer resolution cycles and revenue left on the table.
Plug the Gap:
- Segment A/R by balance size, aging bucket, and payer.
- Prioritize high-yield, short-term aging claims for faster recovery.
- Use automation to trigger payer follow-ups at set intervals (e.g., Day 15, 30, 45).
4. Denials Are Reworked—But Not Resolved
The Problem:
Some teams rework denials without understanding their root cause. A claim might be resubmitted 3 times—without ever fixing the documentation or coding error that caused the first denial.
Why It Matters:
Repetitive rework drains staff time and increases your risk of claim rejection limits. Worse, it creates a false sense of productivity without results.
Plug the Gap:
- Track denials by origin: intake error, provider documentation, billing logic.
- Build feedback loops across departments to correct the upstream issue.
- Hold monthly denial review meetings to monitor recurring trends and fix the workflow, not just the claim.
5. Payer Policy Changes Are Leaving Your Team Behind
The Problem:
Behavioral health payers frequently update authorization requirements, session limits, and documentation rules—but your team doesn’t always catch them in time.
Why It Matters:
Even subtle payer updates (e.g., time-based code limits, treatment plan formats) can lead to denials if your team isn’t adapting quickly.
Plug the Gap:
- Assign a policy lead to monitor changes across your top 10 payers.
- Maintain a shared reference document that is updated weekly.
- Include payer update reviews in your standing RCM meetings.
6. Your Current Billing Partner Isn’t Surfacing Issues
The Problem:
Many outsourced billing companies are reactive, not strategic. They process claims, but they don’t tell you where revenue is leaking—or how to fix it.
Why It Matters:
Without a proactive RCM partner, problems compound. Denials aren’t flagged, authorizations slip, and A/R grows silently until it’s too late to act.
Plug the Gap:
- Require your vendor to provide monthly insight reports—not just billing summaries.
- Ask: What denial trends have you seen? What process improvements do you recommend?
- If your current partner doesn’t offer those insights, it may be time to switch.
7. You’re Not Measuring What Actually Moves the Needle
The Problem:
Most teams track total collections or net revenue—but not the process metrics that drive them. Clean claims rate, average days to submit, and denial overturn success are often missing.
Why It Matters:
You can’t fix what you can’t measure. Without the right KPIs, it’s impossible to tell whether your team is efficient—or just busy.
Plug the Gap:
- Monitor the following metrics weekly:
- First-pass clean claims rate
- Average time to claim submission post-session
- Denial overturn rate
- % of A/R over 60 days
- Use visual dashboards to share trends with leadership.
Behavioral Health RCM Isn’t Just Billing—It’s Strategy
Collections aren’t isolated from care—they’re intertwined. Every missed code, untrained intake staffer, or denial without follow-up ultimately impacts patient services, provider morale, and your ability to grow.
Capture RCM is built to close those gaps.
We don’t just process claims. We work side-by-side with your leadership team to improve collections, shorten A/R cycles, and eliminate the operational friction that’s costing your organization more than just money.
📞 Call (380) 383-6822 or visit our service page to learn how our Behavioral health revenue cycle management services can improve your cash flow, compliance, and peace of mind.
Frequently Asked Questions: Behavioral Health RCM
What’s the most common cause of aging A/R in behavioral health?
Incomplete front-end processes—like missing authorizations, inaccurate patient info, or delayed documentation—are the most common root causes. These create downstream denials that are harder (and slower) to recover.
How can I reduce denials without adding more staff?
Focus on denial prevention through:
- Pre-submission audits
- Payer-specific intake training
- Integrated compliance alerts in your EMR
Many organizations cut denial volume by 20–30% without hiring—just by tightening workflow.
What KPIs should I be tracking to improve collections?
Start with:
- Clean claims rate
- Average days to bill
- Denial overturn rate
- A/R over 60 days
- % of revenue in write-offs
Tracking these monthly can reveal performance gaps early.
How do I know if my billing partner is underperforming?
Warning signs:
- They don’t initiate denial pattern reviews
- Aging A/R grows but reports stay “green”
- You don’t receive documentation improvement feedback
- Denials seem repetitive or unexplained
A strong RCM partner should feel like an extension of your team—not just a vendor.
Can Capture RCM help if we’ve already outsourced billing?
Absolutely. We frequently audit existing vendor relationships, identify underperformance areas, and either optimize or transition the RCM process. Our goal is collections recovery and workflow alignment—whether we’re taking over or enhancing.