

Some days, it’s not census that worries you.
It’s the pending review sitting in someone else’s inbox.
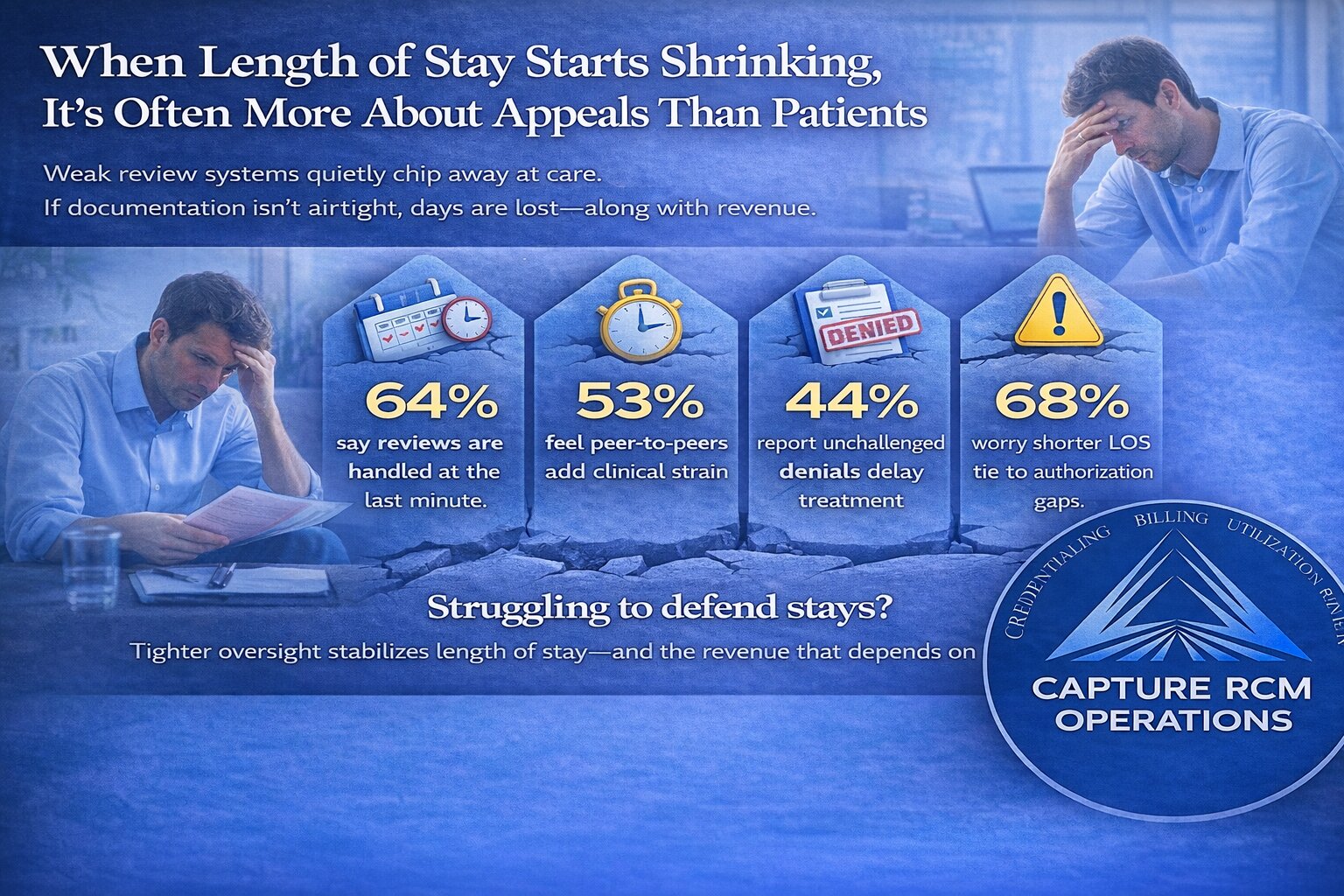
You can feel it before it shows up on the report. Average length of stay dips. Extension approvals get tighter. Denials start creeping in where they didn’t before.
And the hardest part? Clinically, nothing changed.
This is where strong utilization review support becomes more than back-office admin. It becomes clinical protection.
Because when authorizations stall, length of stay shrinks — and that ripple touches everything.
The Slow Erosion of Approved Days
Length of stay rarely collapses overnight.
It fades.
One concurrent review submitted a day late.
One treatment plan that doesn’t clearly connect symptoms to interventions.
One payer who decides progress “should be faster.”
Individually, those moments feel manageable. Collectively, they compress care.
Insurance companies operate on timelines and documentation thresholds. If reviews aren’t scheduled proactively and narratives aren’t tightly aligned with medical necessity criteria, payers default to caution.
That caution shows up as:
- Fewer approved days per review
- Requests for additional documentation
- Step-down pressure before clinical readiness
- Partial denials that chip away at revenue
Over time, your average length of stay drops — not because patients are stabilizing faster, but because oversight wasn’t airtight.
That distinction matters.
When Clinical Momentum Gets Cut Short
Think about what happens clinically when a stay is shortened prematurely.
Patients in PHP or IOP settings often hit a breakthrough right before deeper work begins. Trauma starts surfacing. Family dynamics get unpacked. Medication adjustments are still calibrating.
That work takes time.
When approvals are reduced, the timeline tightens artificially. Instead of completing a stabilization arc, clinicians are forced into discharge planning earlier than expected.
The message patients feel — even if it’s never said out loud — is: Your time is up.
That’s not how recovery should feel.
Length of stay should reflect clinical need, not administrative lag.
Burnout: The Hidden Cost of Weak Review Processes
When review systems are inconsistent, the pressure doesn’t land on leadership first.
It lands on clinicians.
Therapists scrambling to update notes hours before a call.
Clinical directors jumping into last-minute peer-to-peers.
Administrators chasing missing documentation while census keeps moving.
It creates a culture of urgency around something that should be structured.
Over time, that chronic scramble turns into:
- Emotional fatigue
- Defensive documentation habits
- Frustration with “the insurance game”
- Tension between clinical and billing teams
Strong oversight doesn’t just protect revenue. It protects morale.
When review timelines are predictable and documentation standards are clear, your team can focus on care instead of crisis management.
Revenue Compression Happens Quietly
Many operators assume length-of-stay reduction is market-driven.
Sometimes it is.
But often, it’s structural.
Here’s how poor authorization management hurts your numbers:
- Approved days shrink → Average LOS decreases
- Denials increase → AR aging grows
- Appeals are reactive → Recovery rates drop
- Cash flow becomes unpredictable → Growth plans stall
The financial whiplash can feel confusing because census might still look healthy.
But if each patient stays two or three days less than clinically appropriate, the cumulative impact across a month — or quarter — is significant.
And unlike marketing fluctuations, this loss is preventable.
The Difference Between Reactive and Strategic Oversight
There’s a major difference between “handling reviews” and managing them strategically.
Reactive oversight looks like:
- Submitting documentation right before deadlines
- Hoping clinical notes are strong enough
- Appealing only when denials feel obvious
- Escalating issues after authorization has already been cut
Strategic oversight looks different:
- Reviews are calendared before payer deadlines
- Documentation is shaped to mirror medical necessity criteria
- Extension requests are built with forward-looking clinical framing
- Escalation pathways are used early — not after denial
When done correctly, Utilization review services act as a buffer between payer pressure and your clinical team.
They translate clinical progress into payer language.
They anticipate objections before they’re raised.
They defend length of stay with evidence — not emotion.
That defense protects both care and revenue.
Why Payers Reduce Days (Even When Progress Is Real)
It’s important to understand the payer mindset.
Insurance reviewers aren’t in your groups. They don’t see patient affect shift in real time. They don’t witness breakthrough moments in family sessions.
They see documentation.
If notes don’t clearly tie:
- Symptoms → Functional impairment
- Interventions → Measurable response
- Continued stay → Ongoing risk or instability
The default decision leans conservative.
That doesn’t mean your clinical work is weak.
It means the story isn’t being told in the language payers require.
Strong oversight bridges that gap.
Signs Length of Stay Issues May Be Administrative — Not Clinical
If you’re unsure whether LOS shrinkage is structural, ask yourself:
- Has average LOS declined without a change in clinical model?
- Are different reviewers approving different timeframes inconsistently?
- Do you experience sudden step-down pressure late in treatment?
- Are peer-to-peer calls increasing?
- Are appeals rare because they feel time-consuming?
These are signals that your oversight framework may need reinforcement.
None of this means your program isn’t effective.
It means the defense system behind it may be underbuilt.
What Stability Feels Like on the Other Side
When review processes are consistent and proactive, several shifts happen:
- Length of stay stabilizes around clinical benchmarks
- Approval patterns become predictable
- Appeals succeed more often because they’re built correctly
- Clinical staff stop dreading review days
- Cash flow smooths out
The energy inside the facility changes.
Instead of operating from tension, your team operates from clarity.
Instead of reacting to denials, you prevent them.
Instead of losing days quietly, you defend them confidently.
And that confidence compounds over time.
FAQ: Length of Stay & Authorization Oversight
Why does our average length of stay keep dropping?
Often, LOS decline is tied to tighter payer approvals rather than clinical change. If documentation isn’t strategically aligned with medical necessity criteria, insurers may approve fewer days per review cycle.
Can poor review management really impact outcomes?
Yes. When patients discharge earlier than clinically recommended due to authorization limitations, stabilization may be incomplete. This increases the risk of relapse, readmission, and family dissatisfaction.
How early should concurrent reviews be prepared?
Ideally, review prep begins days before the payer deadline. Waiting until the last minute increases documentation gaps and reduces the ability to build a forward-focused extension argument.
Should clinicians handle payer calls themselves?
Clinicians should contribute clinical insight, but they shouldn’t carry the entire authorization burden alone. A structured oversight system ensures calls are supported with strategy, data, and escalation pathways.
Are appeals worth the time?
When built strategically, yes. Many facilities underutilize appeals because they feel administrative and time-consuming. But consistent appeal processes often recover significant revenue and reset approval patterns.
What’s the biggest mistake facilities make with oversight?
Treating it as purely administrative.
Authorization management sits at the intersection of clinical care and revenue protection. When it’s siloed, gaps form. When it’s integrated and strategic, length of stay becomes defensible.
You didn’t build your program to rush people through care. You built it to help them stabilize, heal, and build something sustainable.
If length of stay is shrinking and you can’t explain why, it may not be your treatment model. It may be how your days are being defended.
Call 380-383-6822 or visit our Utilization review services to learn more about our behavioral health billing services.